Post op neuropathy of CP nerve resulting in foot drop
HomeBlogPost op neuropathy of CP nerve resulting in foot drop
Mar 20th, 2024
Post op neuropathy of CP nerve resulting in foot drop
Ming Tan
Medical Imaging Department, Western Health, Footscray, Victoria, Australia
Correspondence
Ming Tan, Medical Imaging Department, Western Health, Melbourne, VIC, Australia.
Introduction
Common peroneal nerve (CPN) neuropathy resulting in foot drop is a relatively uncommon complication of patients who are positioned in the lithotomy position during surgery, and the most common cause of spontaneous painless foot drop.1 Although diagnosis is often based on the clinical findings, ultrasound can be used as an efficient and effective imaging tool to identify the cause of CPN neuropathy and other peripheral nerve disorders. In this article, two ultrasound cases of patients with post operation foot drop as a result of CPN neuropathy are presented. The anatomy, ultrasound imaging technique, ultrasound appearance of CPN neuropathy; and potential causes of CPN are described.
Anatomy of Common Peroneal Nerve
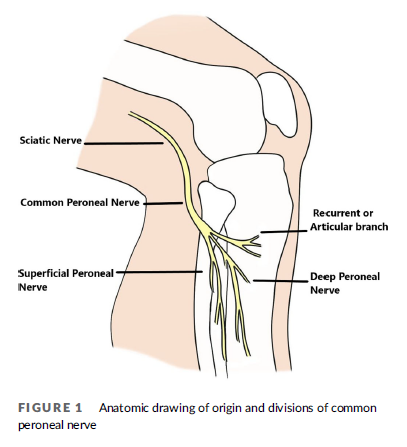
The CPN, also known as the common fibular nerve, is the lateral division of the sciatic nerve (Figure 1). The sciatic nerve bifurcates into the tibial and peroneal nerves proximal to the popliteal fossa.2 The CPN courses from the posterolateral side of the knee around the biceps femoris tendon and the fibular head to enter the lateral compartment of the leg.3 Just inferior and lateral to the fibular head, it divides into three nerves at the fibular neck region including the superficial peroneal nerve, the deep peroneal nerve and a small recurrent articular branch.4
Sonographic Imaging of Common Peroneal Nerve
Ultrasound examination of the CPN involves the use of a high frequency linear transducer. The patient is placed in the prone position. The scan is started at the posterior distal thigh, to identify the sciatic nerve which is then traced inferiorly to its bifurcation. The CPN is the more lateral and smaller branch of the sciatic nerve. The entire length of the CPN is traced to its distal trifurcation at the level of the fibular neck. Colour Doppler can be used to help differentiate nerves from vessels.
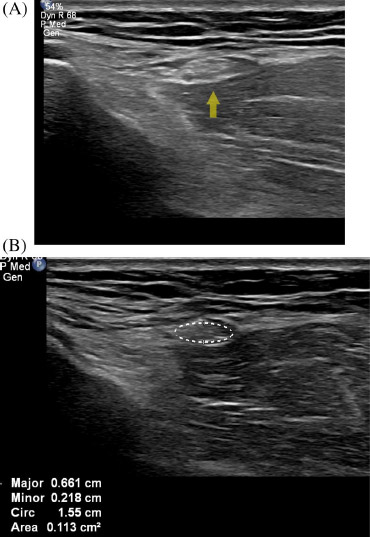
The normal CPN has a ‘honeycomb-like’ appearance in transverse section and a ‘bundle of straws appearance in longitudinal section, which has hypoechoic areas separated by hyperechoic septation. The hypoechoic areas represent nerve fascicles, while the echogenic septation represent interfascicular perineurium, as shown in Figure 2.5–7
FIGURE 1 Anatomic drawing of origin and divisions of common peroneal nerve
FIGURE 2 (A) Normal right common peroneal nerve at the level of the neck of the fibula. Arrow denotes nerve. (B) Normal right common peroneal nerve in cross-section (denoted by ellipse tracing)
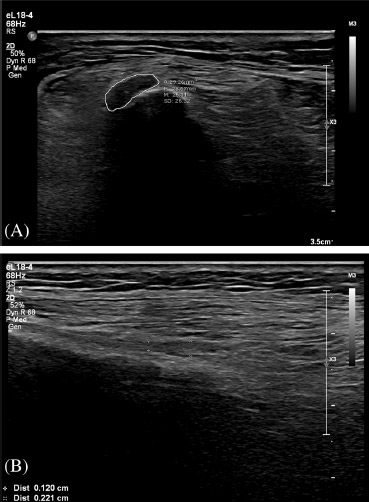
FIGURE 3 Images from a 61-year-old female patient with left foot drop (Case 1). (A) Shows a focally thickened and hypoechoic left CPN at the fibular neck (ellipse tracing). (B) Longitudinal image of common peroneal nerve at the fibular neck demonstrating focal distal thickening
Common Peroneal Nerve Neuropathy Cases
Neuropathy of the CPN can result in foot drop, weakness of other muscles group controlled by the CPN including the extensors of the toes and peroneus muscles and sensory symptoms such as pain and paraesthesia.8 The CPN is responsible for innervating the anterior and lateral muscular compartments of the lower extremity, which include the tibialis anterior muscle, the extensor hallucis longus muscle, and the extensor digitorum longus muscle of the anterior compartment, and the peroneus longus muscle and the peroneus brevis muscle of the lateral compartment. The anterior compartment is responsible primarily for the dorsiflexion of the foot and the lateral compartment is responsible primarily for the eversion of the foot.4 The common site of CPN compression is at the fibula head and neck region.9
Case 1
A 61-year-old female patient presented with newly developed left foot drop, reduced leg muscle power and the sensations of the left leg, at day 7 post left total hip replacement surgery.
Sonography demonstrated a focally thickened and hypoechoic CPN at fibular neck, with a cross-sectional area of 29 mm2 (Figure 3).
Subsequently, the patient reported the foot drop symptoms were resolved after 1 month at outpatient appointment
Case 2
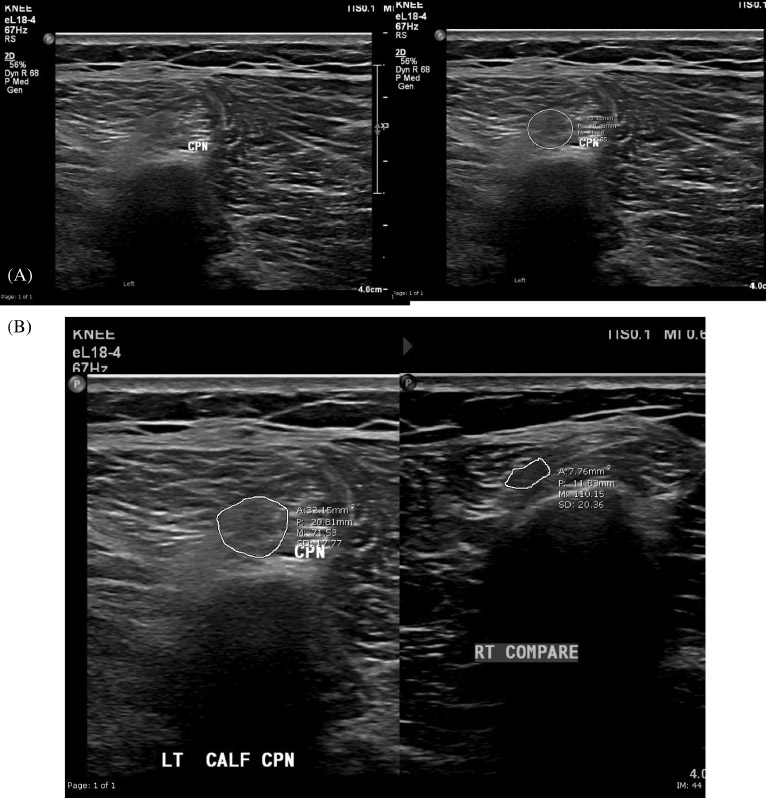
A 27-year-old male patient presented with newly developed left foot drop post open reduction internal fixation surgery of a left proximal tibial fracture. On ultrasound examination, a focal thickening of the CPN at the level of the fibular head was demonstrated. The extensor hallucis longus and extensor digitorum longus tendons appeared intact.
FIGURE 4 Images from a 27-year-old male patient with left foot drop. Sonography demonstrated a focally thickened and hypoechoic CPN at fibular neck, with a cross-sectional area of 33 mm2 . (A) Focally thickened and hypoechoic left common peroneal nerve in cross-section (ellipse tracing). (B) Comparative image of the normal right CPN in cross-section
Sonography demonstrated a focally thickened, oedematous and hypoechoic CPN with a cross-sectional area of 33mm2 (Figure 4).
On follow-up of the orthopaedic clinic review, the patient still presented with minor neurological symptoms of the foot, and the patient was referred for ongoing physiotherapy treatment.
Discussion
In both of these cases, the nerve lost the normal honeycomb-like appearance on ultrasound and became uniformly hypoechoic, which is due to loss of the normal fascicles and damage to the epineurium.10 No colour flow was seen on Doppler ultrasound
The ultrasound images had demonstrated focal thickening of the CPN at the fibular neck with increased cross-sectional areas (Case 1 Figure 3A, 29 mm2 and Case 2 Figure 4A, 33 mm2 ), compared to the normal CPN (Figure 2A). Multiple studies illustrate that upper limit cut-offs values for CPN cross section area ranges from 11.7 to 26.2 mm211–13 and can be used to differentiate normal CPN from neuropathy of CPN. A cut cuff value of 11.7 mm2 has shown a high sensitivity of 85.0% and high specificity of 90.0% from the most recent research.11 Using these criteria, the CPNs described in these two cases are not of normal size
In addition to ultrasound, electrodiagnostic testing, which includes nerve conduction studies (NCS) and needle electromyography (EMG) can be performed to confirm the location of neuropathy.14
Both cases developed CPN neuropathy after orthopaedic surgery. The aetiology of this type of postoperative neuropathy is multifactorial, although most cases are thought to be attributed to patient positioning, compression, or stretching of nerves and inadequate protection of susceptible sites.15 Prolonged compression during orthopaedic, gynaecologic and abdominal surgeries with operative positioning of lateral hip and leg rotation with knee flexion or the lithotomy position can result in peroneal nerve injury. In addition to that, patients who require prolonged bed rest after surgery may also be at risk for peroneal neuropathy.16 Several risk factors have been implicated in lithotomy position-related CPN neuropathy during operation. When the CPN exits the popliteal fossa, the common peroneal nerve crosses the lateral head of gastrocnemius and popliteus and wraps around the fibula neck in order to enter the lateral compartment of the leg.17 Around this area, the CPN is exposed over a bony prominence covered superficially only by subcutaneous fat and skin for a length of 4 cm. The CPN also has limited longitudinal mobility where the nerve is in a relatively fixed position from its origin at the sciatic nerve to the trifurcation at the level of the fibular neck. All these factors together make the CPN susceptible to external compression or other injury over this region.9,18,19
To help to reduce the incidence of neuropathy of the CPN, for operations with patients in the lithotomy position, or other positions that involve fixation of the leg, the fixing duration should be reduced in order to prevent postoperative neurologic complications.20 Studies illustrate that the risk of motor neuropathy is increased by 100 times as the external fixation time increases by 1 h.18,21
The symptoms of the patient in case 1 resolved after 1 month. For case 2 the patient’s symptoms had nearly resolved after been treated with physiotherapy for 4 months. Studies have demonstrated that there are high rates of spontaneous recovery of CPN palsy with conservative management in cases where the causative mechanism was compression.9
Many patients will experience spontaneous recovery early in the course, and hence observation and symptomatic treatment is the first line of management. For those patients who do not spontaneously improve, surgical decompression is a safe and effective treatment option.4,22
Conclusion
Post-operative neuropathy of CPN resulting in foot drop is a rare surgical complication. It is commonly caused by prolonged compression of the CPN at the region of neck of fibular from the fixed position. Ultrasound can effectively assess CPN neuropathy in patients with foot drop. Although CPN neuropathy will recover spontaneously in most patients, surgical decompression should be considered for patients with persistent neuropathy.
Acknowledgments
The author would like confirm upon submission that informed consent to publish has been obtained from the patients who are involved in this case study and thanks for the patients’ support of the writing and publishing of this case study. The Author would like to express his special thanks and acknowledge the help and contribution of: Mr Adam Steward, Radiography Tutor of Western Health Medical Imaging Department and Ms Renee Mineo, General Radiography Supervisor of Western Health Medical Imaging Department, for the internal reviews of the article. Ms Nicole McDonald, Chief Sonographer of Western Health Medical Imaging Department and Mr Jason Heidrich Chief Radiographer of Western Health Medical Imaging Department Footscray Hospital, for approval and support of the article. Ms Sandra McConville, Clerical Supervisor of Western Health Medical Imaging Department, for help obtain the written consent. Miss Yongying Han, author’s fiancée, for the illustrate drawing of the anatomy of the common peroneal nerve.
Funding Information
The article is founded by Western Health Medical Imaging Department, Victoria
Conflict Of Interest Statement
The authors declare that they have no conflicting interests.
Informed Consent
Recorded informal consents were obtained from the patients, for the purpose of publication of this case report and any accompanying images.
Capodici A, Hagert E, Darrach H, Curtin C. An overview of common peroneal nerve dysfunction and systematic assessment of its relation to falls. Int Orthop. 2022;46(12):2757–63. https://doi.org/10.1007/ s00264-022-05593-w
Van den Bergh FR, Vanhoenacker FM, De Smet E, Huysse W, Verstraete KL. Peroneal nerve: normal anatomy and pathologic 4 TAN findings on routine MRI of the knee. Insights Imaging. 2013;4(3): 287–99. https://doi.org/10.1007/s13244-013-0255-7
Hardin JM, Devendra S. Anatomy, bony pelvis and lower limb, calf common peroneal (fibular) nerve. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 [Updated 2022 Oct 17].
Lawande AD, Warrier SS, Joshi MS. Role of ultrasound in evaluation of peripheral nerves. Indian J Radiol Imaging. 2014;24(3):254–8. https://doi.org/10.4103/0971-3026.137037
Berry H, Richardson PM. Common peroneal nerve palsy: a clinical and electrophysiological review. J Neurol Neurosurg Psychiatry. 1976; 39(12):1162–71. https://doi.org/10.1136/jnnp.39.12.1162
Cartwright MS, Walker FO. Neuromuscular ultrasound in common entrapment neuropathies. Muscle Nerve. 2013;48(5):696–704. https://doi.org/10.1002/mus.23900
Kim JY, Song S, Park HJ, Rhee WI, Won SJ. Diagnostic cutoff value for ultrasonography of the common fibular neuropathy at the fibular head. Ann Rehabil Med. 2016;40(6):1057–63. https://doi.org/10. 5535/arm.2016.40.6.1057
Cruz-Martinez A, Arpa J, Palau F. Peroneal neuropathy after weight loss. J Peripher Nerv Syst. 2000;5:101–5.
Lo YL, Fook-Chong S, Leoh TH, Dan YF, Tan YE, Lau WH, et al. Highresolution ultrasound as a diagnostic adjunct in common peroneal neuropathy. Arch Neurol. 2007;64:1798–800.
Novello BJ, Pobre T. Electrodiagnostic evaluation of peripheral neuropathy. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 [Updated 2022 Oct 3].
Mizuno J, Takahashi T. Factors that increase external pressure to the fibular head region, but not medial region, during use of a knee-crutch/leg-holder system in the lithotomy position. Ther Clin Risk Manag. 2015;16(11):255–61. https://doi.org/10.2147/TCRM. S72511
Marciniak C. Fibular (peroneal) neuropathy: electrodiagnostic features and clinical correlates. Phys Med Rehabil Clin N Am. 2013;24(1):121– 37. https://doi.org/10.1016/j.pmr.2012.08.016
Gruber H, Peer S, Meirer R, Bodner G. Peroneal nerve palsy associated with knee luxation: evaluation by sonography—initial experiences. AJR Am J Roentgenol. 2005;185(5):1119–25. https://doi.org/ 10.2214/AJR.04.1050
Grant TH, Omar IM, Dumanian GA, Pomeranz CB, Lewis VA. Sonographic evaluation of common peroneal neuropathy in patients with foot drop. J Ultrasound Med. 2015;34(4):705–11. https://doi.org/10. 7863/ultra.34.4.705
Chung JH, Ahn KR, Park JH, Kim CS, Kang KS, Yoo SH, et al. Lower leg compartment syndrome following prolonged orthopedic surgery in the lithotomy position: a case report. Korean J Anesthesiol. 2010;59 Suppl(Suppl):S49–52. https://doi.org/10.4097/kjae.2010. 59.S.S49
Warner MA, Warner DO, Harper CM, Schroeder DR, Maxson PM. Lower extremity neuropathies associated with lithotomy positions. Anesthesiology. 2000;93(4):938–42. https://doi.org/10. 1097/00000542-200010000-00010
Wijntjes J, Borchert A, van Alfen N. Nerve ultrasound in traumatic and iatrogenic peripheral nerve injury. Diagnostics (Basel). 2020; 11(1):30. https://doi.org/10.3390/diagnostics11010030
How to cite this article: Tan M. Post operation neuropathy of common peroneal nerve resulting in foot drop. Sonography. https://doi.org/10.1002/sono.12359
Really efficient and friendly service, comfortable environment. Highly Recommended.I'm also just super grateful that l can have these types of scans done under Medicare....
Shehal Gomes
1747723899
I’ve been to Precise Radiology a couple of times now (ultrasound, xray etc) and each time has been super smooth. Shoutout to Renee at the front desk, she’s fantastic. The team’s great and everything runs on time. Highly recommend!
Helen Young
1747112207
The staff at Precise Radiology are amazing!
Lexi
1746830898
Had a great experience at Precise Radiology. The staff were friendly and professional. A special thanks to Ming—he was very patient, gentle, and explained everything clearly. I felt well taken care of and reassured throughout the ultrasound scan. Highly recommend!!
Wendy Moore
1745803476
Very lovely staff members welcoming and professional and a comfortable relaxing atmosphere while waiting in the waiting area.
Nadia kootab
1744711224
This place is incredible. Highly recommend for anyone looking for compassionate and professional care.
Kara S
1743311020
Great staff and service at precise radiology. I have been twice in the past month and would highly recommend
Jackie
1742349200
I had an outstanding experience at Precise Radiology Carnegie! This morning, my doctor referred me for a bone densitometry scan, and since I had taken time off work, I wanted to get it done the same day. Most radiology centres required an advance booking and quoted me $160 with no bulk-billing. Just as I was about to give up, I found Precise Radiology Carnegie online and gave them a call.Chris was incredibly helpful and managed to fit me in on the same day while offering a more affordable price than other places. From the moment I arrived, I was impressed—the waiting area had a unique setup, the clinic was spotless, and it even smelled nice! The radiologist, Steven, was caring, personable, and truly dedicated to his role. The new patient questionnaire was clear and easy to complete.Although I didn’t expect my scan to be bulk-billed, both Steven and Chris went the extra mile to check with Medicare, and my scan ended up being mostly rebated—a fantastic bonus! I genuinely appreciate their effort and professionalism.I can’t believe this radiology centre has been around for three years, and I’m only discovering it now. I’ll definitely return for any future imaging needs and happily recommend them to others. Highly recommend!
Mariam Mousa
1742346395
Great service. Feels like a day spa. Ming is extremely professional and experienced and put me at ease the whole time.
Tiffany Tra
1741320980
Scott and his team were fantastic. When my dad needed an urgent CT scan, they accommodated him the same afternoon. Having Anh there to translate into Vietnamese was incredibly helpful, ensuring dad fully understood the process. The team took the time to explain everything clearly, and the reception staff were warm and welcoming. The entire experience was smooth and efficient. I'll definitely be returning for any future scans!
Karen Vera
1741220499
The lady at the front office was amazing—kind, helpful, and welcoming. The doctors were also very gentle and attentive, making the experience even better!
Rosmery Alfonso
1741130793
Amazing facilities and service. Super quick and easy.
CHUNG YOON HAN
1741081423
I didn’t realize my finger was broken and tried to tough it out, but my GP advised me to get an X-ray as soon as possible. I attempted to make appointments at several places, but all of them were fully booked. (If I tried full booking or submitted an online booking request, I would get a call, but I couldn’t answer. When I called back, the staff told me to come the next day.) Fortunately, the last place I visited, Precise Radiology Carnegie, was incredibly friendly and quick. What I especially appreciated was that when I submitted an online booking request, they emailed me saying that X-rays could also be done as a walk-in, which I was very grateful for.
Charlotte Haddad
1741069762
Always helpful, accurate and attentive. I am always guaranteed a spot.
Mauhameden Elycheikh
1741035269
Liam McGill
1740984780
Scott and the team at Precise Radiology are welcoming and professional. Walking through the door you feel a sense of trust and assurance you'll be looked after, and that's what you'll get at this facility. Recommend using their services highly!
Clean N' Co Services
1740984463
Nicky Auster Gafni
1740708955
I never thought I’d say this about getting a CT Scan but the customer service was outstanding! They fitted me in the same day and the staff were very professional and caring, explaining everything patiently the whole way. Steven, the radiographer was excellent, explaining the procedure in detail before and after. Plus it was bulk billed. Highly recommended!
Rachelle Wang
1740625881
Really happy with my experience there, the sonographer lady Celia was amazing, she was gentle and very thorough with the checks, she also explained everything in the way that I could understand. I did two ultrasound there during my first trimester pregnancy, felt very well looked after. Will recommend it to my friends!
Xyrx Quemuel
1740616533
Tatyana Dikshteyn
1740533782
Fast service. Nice cosy atmosphereBulk billed or good prices
Alam Usa
1738282866
The best service obstetric ultrasound.Professional and cooperative staff. Recommend to everyone. We traveled Melton - Carnegie (80km)for their incredible service
Wayne Quirk
1737621546
As a Health professional I was extremely impressed with the efficient polite and courteous nature of all the staff that I came in contact with at precise Radiology. I couldn’t recommend them more highly. Keep up the good work!
Bianca Melb
1735699448
I needed an urgent Xray because I was flying back home to Cairns later that afternoon. And a lot of places were closed because it was between Christmas and NY, so we were relieved Precise were open. Not only were they professional, the report and results were sent to my GP within 3 hours. It was a very well presented practice too, so clean and comfortable. Highly recommended
Damien Henneken
1734675732
Every client I asked for them to fit or take care of they did without exception. Precisely what Donna Maree said, exactly what Carnegie needed.
bhasker goud
1734616182
Very quick to book an appointment and very good customer service.
Kaz Petrulyte
1734146943
The admin staff and the technician are so lovely, caring and professional. The clinic itself is also very peaceful with low lighting which is very appreciated. Highly recommended
Zakary Doherty
1733896636
Gary Chan
1731994633
Jeffrey Chang
1731569554
Came here because of the google review rating. Was not disappointed!
Lily J
1730615454
Fantastic clinic, staff are so friendly and helpful.
Vera Teodori
1729744563
donna maree
1729418190
Precisely what Carnegie needed! This clinic offers a range of bulk billed services with referral based walk in appointments. Clean modern facilities in Carnegie Central shopping centre.
Sandy Archer
1728878986
I had a CT guided epidural and the care and compassion was outstanding. I was told every step of what was being done throughout the procedure. I traveled from Rye as heard good reports about this practice. Thank you Ahn and the doctor (sorry forgot his Name) the experience was very comforting.
sarah hussein
1727829880
Excellent service. I’ve been coming here for over a year now and always do my scans with Celia. Staff is very friendly and helpful.highly recommended🙏
Liz S
1727788363
From my first contact with this company I had a good feeling. The guy on the phone (sorry didn’t catch his name) was polite, helpful, answered all my questions and was able to get us in urgently. On arrival at the facility, again staff were attentive and friendly. What a breath of fresh air. I wish they could sprinkle some of their ‘happy dust’ on most other medical clinics. It’s so rare to have such a positive experience from beginning to end. Someone needs to recognise these employees and thank them for representing the company so well.
Bindi Kamal
1727758936
Fantastic service by all the staffs and receptionist is always very helpful.
Tysen Woodlock
1727320588
I had a calcium score test which is an out of pocket test. Precise Radiology is between $50 to as much as $100 cheaper than the other clinics. The staff were friendly and professional.
Natasha Garfinkel
1727074396
Fat Chop
1726214211
Fantastic staff and service.
F Z
1726204727
Did both ultra sound on the same day, Everyone in this clinic is friendly and nice. Definitely will recommend the radiology to others!
Shaun Richardson
1726052440
Fantastic radiology clinic. Have sent multiple patients here and have been impressed with the quality of reporting - so much so that I've occasionally sent to this clinic for second opinions when other radiology clinics provided insufficient detail in their reports.Highly recommend, very happy referrer.
Claire Richardson
1726052048
I am a local Osteopath and refer many patients to Precise. I have also attended as a patient myself, and taken my baby here.I have always been impressed with the professionalism of the staff at Precise.The clinic is clean and modern, they are able to accommodate important scans quickly, the reception staff are polite, and most importantly, their radiography team are immensely knowledgeable and kind.Will continue to recommend my patients attend Precise if they require medical imaging.
Sebastian Bonilla Tangarife
1725674126
Everything was so good and the receptionist was the best. Very helpful despite she was very very busy. Good clinic willing to help you.
Meme Z
1724722047
happy with the visit. ultrasound was bulkbilled for medicare card holders. itwas an intern student who did my scan but was checked up by the supervisor afterwards. called up on Friday and got an appointment the following Monday which is quick.
Ania Nguyen
1724123514
Amazing (same day) service, lovely and caring staff, on time and incredibly professional service. Would highly recommend to anyone who needs urgent imaging tests.
Darren Tannen
1723943996
I went to Precise Radiology Carnegie for an x ray and an ultrasound for my knee. The staff are amazing. They are very polite,friendly and professional. The ultrasound technician was very polite and friendly. The radiologic technologist was very professional and helpful.I highly recommend Precise Radiology Carnegie
Vinay Krishnan
1723769985
The precise radiology staff are some of the best in the business. The professionalism and care they have for patients is held in high regard. They go above and beyond to make you feel cared for and have some of the latest cutting edge medical imaging equipment including their new Philips CT scanner. Highly recommend anyone else looking to get their medical imaging needs looked after, to be done correctly and done precisely at Precise Radiology!
 Same Day Reporting Available
Same Day Reporting Available